CCM (Continuous Conduction Mode) and DCM (Discontinuous Conduction Mode) are two operational modes of power converters that impact efficiency, ripple, and component stress differently based on current flow characteristics. Discover how understanding these modes can optimize your power supply design and performance by reading the rest of the article.
Table of Comparison
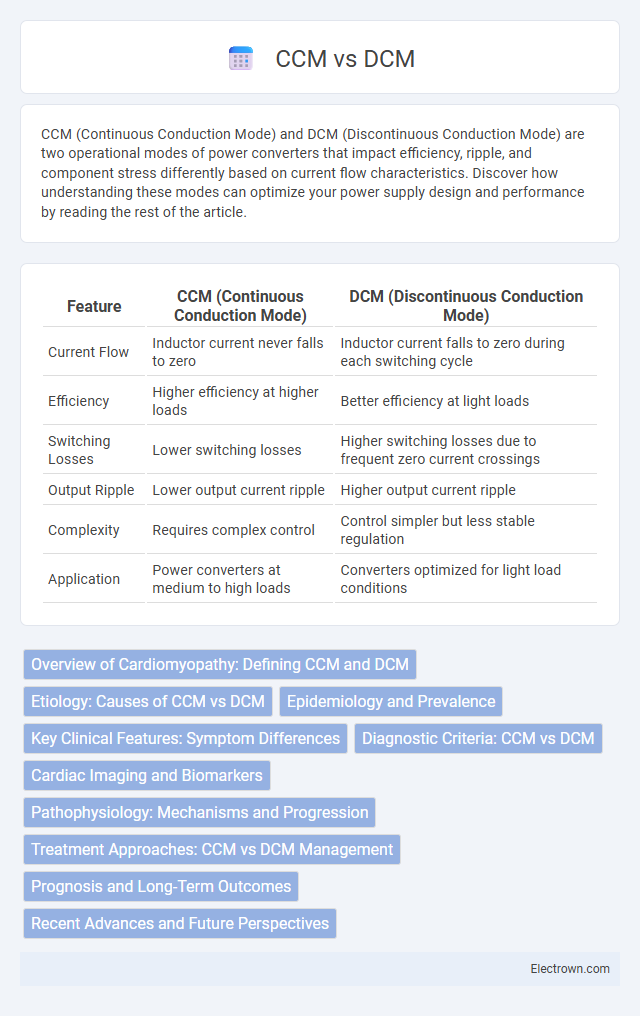
| Feature | CCM (Continuous Conduction Mode) | DCM (Discontinuous Conduction Mode) |
|---|---|---|
| Current Flow | Inductor current never falls to zero | Inductor current falls to zero during each switching cycle |
| Efficiency | Higher efficiency at higher loads | Better efficiency at light loads |
| Switching Losses | Lower switching losses | Higher switching losses due to frequent zero current crossings |
| Output Ripple | Lower output current ripple | Higher output current ripple |
| Complexity | Requires complex control | Control simpler but less stable regulation |
| Application | Power converters at medium to high loads | Converters optimized for light load conditions |
Overview of Cardiomyopathy: Defining CCM and DCM
Cardiomyopathy encompasses a group of diseases affecting the heart muscle, with CCM (Chronic Chagas Cardiomyopathy) and DCM (Dilated Cardiomyopathy) representing distinct forms. CCM is caused by the Trypanosoma cruzi infection leading to chronic inflammation and myocardial damage, predominantly in Latin America. DCM is characterized by ventricular dilation and impaired systolic function without ischemic or valvular causes, resulting in progressive heart failure and arrhythmias.
Etiology: Causes of CCM vs DCM
Chronic Chagas myocarditis (CCM) is primarily caused by infection with the protozoan parasite Trypanosoma cruzi, which is transmitted by triatomine bugs endemic to Latin America, leading to an inflammatory cardiomyopathy. Dilated cardiomyopathy (DCM) has a more heterogeneous etiology, including genetic mutations affecting sarcomeric or cytoskeletal proteins, viral infections such as enteroviruses or adenoviruses, and toxic exposures like alcohol or chemotherapy agents. Understanding your specific cause is crucial for accurate diagnosis and targeted treatment strategies in these cardiomyopathies.
Epidemiology and Prevalence
Chronic Chagas cardiomyopathy (CCM) affects approximately 20-30% of individuals infected with Trypanosoma cruzi, predominantly in Latin America, where an estimated 6-7 million people are infected. Dilated cardiomyopathy (DCM) has a global prevalence of about 1 in 250 adults and is a leading cause of heart failure and heart transplants worldwide. The geographic distribution and etiologies differ, with CCM closely linked to endemic areas of Chagas disease, while DCM arises from diverse causes including genetic, infectious, and toxic factors.
Key Clinical Features: Symptom Differences
CCM (Cerebral Cavernous Malformation) commonly presents with seizures, headaches, and focal neurological deficits due to intermittent hemorrhages, whereas DCM (Degenerative Cervical Myelopathy) typically manifests as progressive limb weakness, numbness, gait instability, and fine motor skill deterioration caused by spinal cord compression. Unlike CCM, which often has sudden episodic symptoms associated with vascular malformations visible on MRI, DCM symptoms develop gradually and worsen over time with degenerative changes in the cervical spine. Clinical differentiation relies heavily on symptom onset patterns and neurological examination findings tailored to lesion location and disease pathophysiology.
Diagnostic Criteria: CCM vs DCM
CCM (Cardiomyopathy) diagnosis is primarily based on imaging techniques such as echocardiography and MRI, revealing ventricular dilation and systolic dysfunction without significant coronary artery disease, whereas DCM (Dilated Cardiomyopathy) diagnosis also relies on these imaging modalities but emphasizes left or both ventricular enlargement and impaired contractile function with exclusion of other causes like hypertension or valvular disease. Biomarkers like BNP and genetic testing often support the differentiation by identifying underlying etiologies in both conditions. Endomyocardial biopsy or advanced genetic panels may be utilized for further specificity in CCM compared to the broader clinical exclusion process seen in DCM diagnosis.
Cardiac Imaging and Biomarkers
Cardiac imaging techniques such as echocardiography and MRI provide critical insights into left ventricular function, allowing differentiation between continuous conduction monitoring (CCM) and discontinuous conduction monitoring (DCM) by assessing myocardial strain and ejection fraction. Biomarkers like BNP and troponin levels further enhance diagnostic accuracy by indicating myocardial stress and injury, which are more continuously tracked in CCM due to its real-time data acquisition. Your personalized cardiac assessment benefits from integrating these imaging modalities and biomarker trends to optimize monitoring strategies and treatment plans.
Pathophysiology: Mechanisms and Progression
Chronic Chagas cardiomyopathy (CCM) results from persistent Trypanosoma cruzi infection causing myocardial inflammation, fibrosis, and autonomic nervous system damage leading to left ventricular dysfunction and arrhythmias. In contrast, dilated cardiomyopathy (DCM) involves genetic mutations or acquired insults causing myocardial cell injury, dilation of cardiac chambers, and systolic dysfunction without infectious etiology. The progression of CCM is characterized by a chronic inflammatory response and immune-mediated myocardial damage, whereas DCM progression is primarily associated with cardiomyocyte apoptosis and remodeling.
Treatment Approaches: CCM vs DCM Management
Continuous Conduction Mode (CCM) and Discontinuous Conduction Mode (DCM) require distinct treatment approaches for optimal management. CCM involves designing control strategies to handle ripple current and maintain steady-state performance, often utilizing current-mode control to enhance efficiency. Your choice between CCM and DCM management depends on factors like load conditions and electromagnetic interference requirements, ensuring stable operation and efficient power delivery.
Prognosis and Long-Term Outcomes
CCM (Chronic Cerebral Methamphetamine) users often face more severe cognitive decline and a higher risk of neurodegenerative disorders compared to DCM (Dilated Cardiomyopathy) patients, who primarily contend with progressive heart failure and arrhythmias. Long-term outcomes in CCM cases are frequently marked by persistent neurological deficits and increased mortality due to vascular complications, whereas DCM prognosis depends largely on cardiac function improvement with medical or device therapy. Survival rates and quality of life for DCM have improved due to advancements in pharmacologic treatment and heart transplantation options, contrasting with limited recovery prospects in CCM-related brain damage.
Recent Advances and Future Perspectives
Recent advances in CCM (Continuous Conduction Mode) and DCM (Discontinuous Conduction Mode) focus on improving power efficiency and minimizing electromagnetic interference in power converters. Innovations in digital control algorithms and wide-bandgap semiconductor devices enable superior performance in both modes under varying load conditions. Future perspectives emphasize adaptive mode control strategies and integration with advanced materials to enhance reliability and reduce energy losses in renewable energy and electric vehicle applications.
CCM vs DCM Infographic