Lead I records the electrical activity between the right and left arms, providing a lateral view of the heart, while Lead II measures between the right arm and left leg, offering a more inferior perspective and clearer depiction of the P wave and rhythm. Understanding these differences can enhance your interpretation of ECG readings for accurate cardiac assessment; continue reading to explore their clinical significance and practical applications.
Table of Comparison
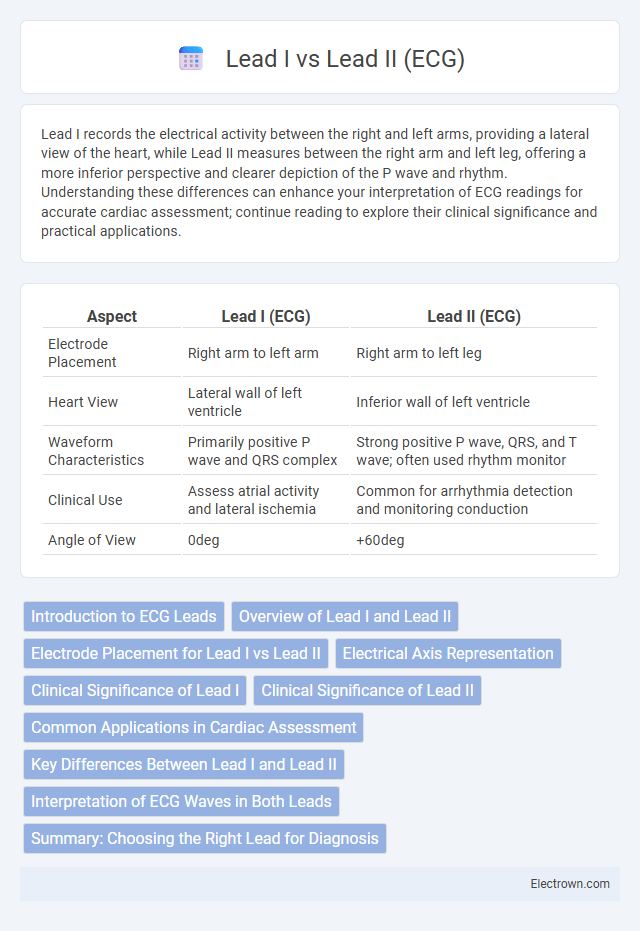
| Aspect | Lead I (ECG) | Lead II (ECG) |
|---|---|---|
| Electrode Placement | Right arm to left arm | Right arm to left leg |
| Heart View | Lateral wall of left ventricle | Inferior wall of left ventricle |
| Waveform Characteristics | Primarily positive P wave and QRS complex | Strong positive P wave, QRS, and T wave; often used rhythm monitor |
| Clinical Use | Assess atrial activity and lateral ischemia | Common for arrhythmia detection and monitoring conduction |
| Angle of View | 0deg | +60deg |
Introduction to ECG Leads
Lead I records the electrical activity of the heart between the right arm and left arm electrodes, capturing lateral heart wall signals predominantly from the left atrium and ventricle. Lead II measures the potential difference between the right arm and left leg electrodes, providing a view aligned with the heart's natural electrical axis, often yielding the clearest P wave for atrial activity analysis. These leads are fundamental in a 12-lead ECG setup, enabling comprehensive assessment of cardiac rhythm, ischemia, and conduction abnormalities by offering complementary anatomic perspectives.
Overview of Lead I and Lead II
Lead I records the electrical activity of the heart between the right arm and left arm electrodes, providing a lateral view of atrial and ventricular depolarization. Lead II captures the signal from the right arm to the left leg, offering a more inferior perspective and often producing the most prominent P waves and QRS complexes. Understanding the distinct orientations of Lead I and Lead II helps you interpret cardiac rhythms and identify arrhythmias accurately.
Electrode Placement for Lead I vs Lead II
Lead I electrode placement involves positioning the right arm electrode on the right wrist or shoulder and the left arm electrode on the left wrist or shoulder, creating a horizontal electrical view of the heart. Lead II electrode placement uses the right arm electrode on the right wrist or shoulder and the left leg electrode on the left lower torso or ankle, capturing a diagonal axis from the right arm to the left leg. Your understanding of these placements helps accurately interpret ECG waveforms for cardiac assessment.
Electrical Axis Representation
Lead I and Lead II in ECG represent different perspectives of the heart's electrical axis, with Lead I measuring the electrical activity horizontally across the heart from right to left, capturing the heart's lateral view. Lead II records the electrical flow diagonally from the right arm to the left leg, aligning closely with the heart's natural depolarization vector, providing a comprehensive view of the inferior heart wall. Accurate interpretation of these leads aids in determining the heart's mean electrical axis, crucial for diagnosing axis deviations and related cardiac conditions.
Clinical Significance of Lead I
Lead I in an ECG provides critical information about the electrical activity of the lateral part of the heart, particularly the left atrium and left ventricle, making it essential for identifying atrial enlargement and left ventricular hypertrophy. Compared to Lead II, which is often favored for rhythm monitoring due to its alignment with the heart's electrical axis, Lead I offers unique diagnostic value in detecting ischemia in the high lateral wall of the left ventricle. Your assessment of Lead I can enhance the detection of abnormalities such as left atrial enlargement and lateral myocardial infarction, improving clinical decision-making and patient outcomes.
Clinical Significance of Lead II
Lead II in electrocardiography provides a clear view of the heart's electrical activity along the inferior wall, making it crucial for detecting arrhythmias such as atrial fibrillation and identifying inferior myocardial infarction. Compared to Lead I, Lead II aligns closely with the heart's natural conduction pathway, offering superior sensitivity for monitoring P wave morphology and rhythm interpretation. Its clinical significance lies in its ability to facilitate continuous rhythm monitoring and early diagnosis of cardiac abnormalities during stress testing and ambulatory ECG recordings.
Common Applications in Cardiac Assessment
Lead I and Lead II in ECG are essential for cardiac rhythm analysis and detecting atrial abnormalities. Lead I is primarily used for identifying atrial enlargement and lateral wall ischemia, while Lead II excels in monitoring cardiac arrhythmias due to its alignment with the heart's electrical axis. Both leads are routinely employed in stress testing, ambulatory Holter monitoring, and early diagnosis of myocardial infarction.
Key Differences Between Lead I and Lead II
Lead I records the electrical activity between the right arm and left arm, primarily capturing lateral heart wall signals, while Lead II measures between the right arm and left leg, highlighting inferior heart wall activity. Lead II typically shows a stronger P wave and QRS complex due to alignment with the heart's natural electrical axis, making it ideal for rhythm analysis and arrhythmia detection. Your ECG interpretation benefits from understanding these differences, as Lead I offers a lateral perspective and Lead II provides a clearer view of atrial and ventricular depolarization.
Interpretation of ECG Waves in Both Leads
Lead I in ECG primarily shows electrical activity between the right and left arms, emphasizing the horizontal plane and providing clear P wave, QRS complex, and T wave patterns for atrial and ventricular events. Lead II captures electrical signals between the right arm and left leg, aligning closely with the heart's natural conduction axis, making it optimal for detecting P wave morphology and identifying arrhythmias. Differences in wave amplitude and morphology between Lead I and Lead II assist clinicians in diagnosing atrial enlargement, conduction delays, and axis deviations with higher accuracy.
Summary: Choosing the Right Lead for Diagnosis
Lead I records electrical activity between the right and left arms, ideal for detecting atrial abnormalities and lateral wall ischemia, while Lead II captures signals from right arm to left leg, providing clearer insights into heart rhythm and inferior wall infarctions. Your choice depends on the clinical focus: Lead II offers superior visualization of P waves for arrhythmia diagnosis, whereas Lead I enhances detection of ischemic changes in the lateral myocardium. Accurate ECG interpretation requires selecting the lead that best highlights the suspected cardiac condition.
Lead I vs Lead II (ECG) Infographic